Gastroshiza: Understanding, Managing, and Living Beyond It
Few words can cause more concern for parents-to-be than hearing the term gastroshiza during a prenatal check-up. It is a condition that often raises urgent questions: What does this mean for my baby? Is it treatable? Can my child live a normal life? These fears are natural, and the purpose of this article is to address them with clarity, compassion, and evidence-backed information.
I still remember a close family friend facing this diagnosis during her pregnancy. The first weeks were filled with confusion, but after proper guidance, her child underwent surgery and today lives a healthy, active life. This is a testament to how far medical science has come in treating gastroshiza and why awareness plays a crucial role in navigating it.
This guide combines real-world insight, medical expertise, and practical advice. By the end, you will understand not only what gastroshiza is, but also how it is diagnosed, treated, and managed for a brighter future.
What is Gastroshiza?
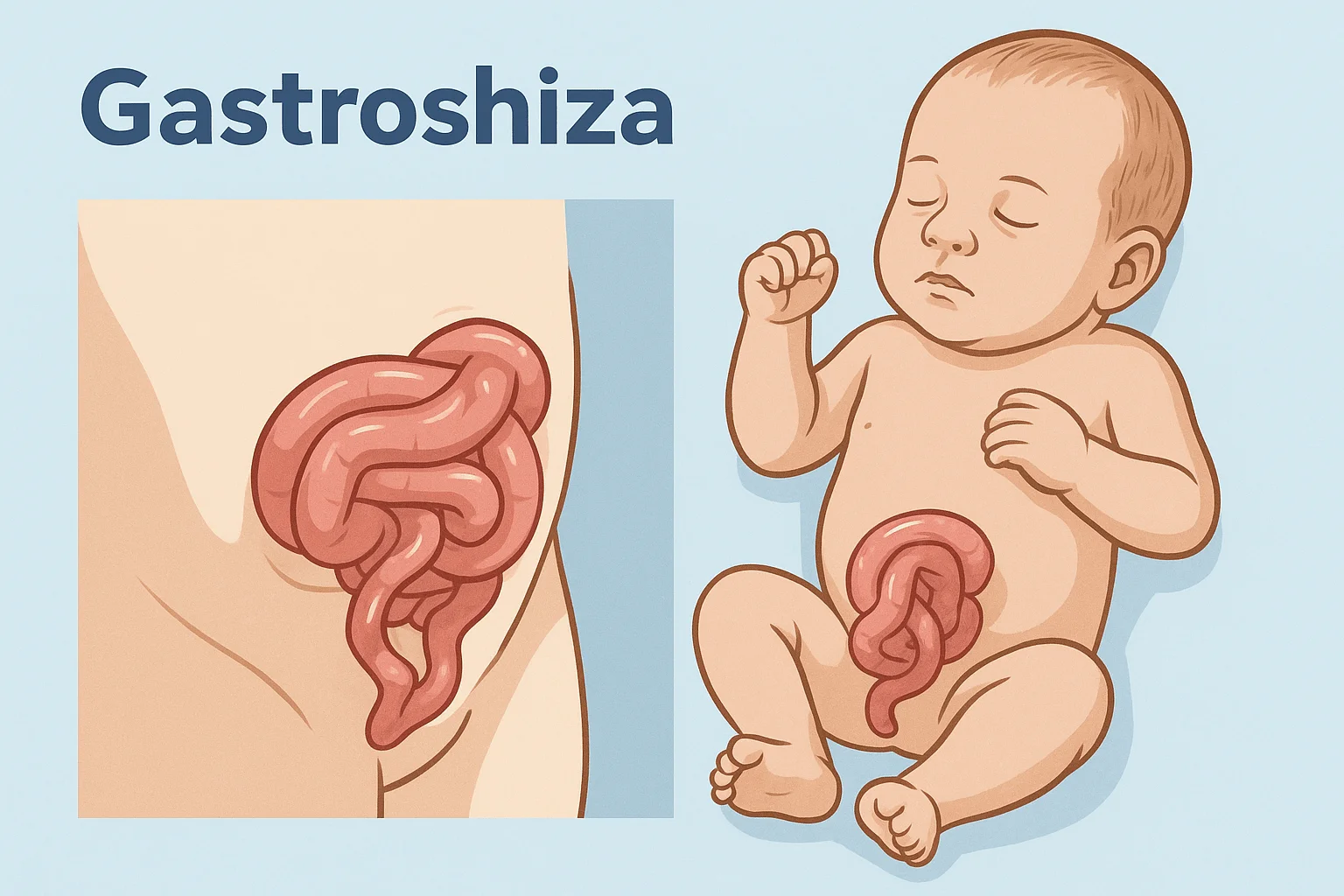
Gastroshiza is a birth defect where a baby is born with their intestines protruding outside the abdominal wall through a small opening near the belly button. Unlike other abdominal wall defects, such as omphalocele, gastroshiza typically occurs without a protective sac around the exposed organs, making immediate medical attention essential.
Doctors usually detect it during routine prenatal ultrasounds, often between 18–22 weeks of pregnancy. According to pediatric surgical research, the condition occurs in about 1 in every 2,000–4,000 live births, with varying prevalence across regions.
Why Understanding Gastroshiza Matters Today
Over the past two decades, survival rates for infants born with gastroshiza have dramatically improved. In advanced healthcare systems, survival can exceed 90%. However, the challenge lies in global disparities—while some countries offer cutting-edge surgical care, others struggle with access to neonatal intensive care.
Rising awareness also helps expectant parents emotionally prepare. Unlike past generations where knowledge was scarce, today families can benefit from online communities, support groups, and multidisciplinary medical teams.
Causes and Risk Factors
Medical experts do not fully agree on a single cause of gastroshiza, but several factors are associated with increased risk:
- Maternal Age: Studies show a higher occurrence in mothers under 20 years old.
- Lifestyle Factors: Smoking, alcohol, and certain drug exposures during pregnancy may increase risks.
- Environmental Exposure: Agricultural chemicals and urban pollutants have been suggested as possible contributors.
- Genetic Links: Unlike some congenital conditions, gastroshiza usually isn’t inherited, though ongoing research continues.
It’s important to emphasize that parents should never blame themselves. Most cases arise without clear prevention measures, and focusing on medical solutions remains the most constructive path.
Diagnosis and Early Detection
Prenatal screening plays a critical role in managing gastroshiza. The two main methods are:
- Ultrasound Scans – The condition is usually visible on a standard mid-pregnancy scan, showing the intestines outside the abdomen.
- Maternal Serum Alpha-Fetoprotein (MSAFP) Test – Higher-than-normal levels may suggest abdominal wall defects.
Early detection allows families to plan for delivery in a specialized hospital with neonatal intensive care and pediatric surgeons available immediately after birth.
Treatment Options
Treatment of gastroshiza always requires surgery, but the approach depends on the severity.
Primary Repair
If the abdominal opening is small and the baby’s intestines are not severely swollen, doctors may perform a primary closure, placing the intestines back inside and sealing the abdominal wall during a single surgery.
Staged Repair
In more complex cases, surgeons use a silo bag—a sterile pouch that gradually reintroduces the intestines into the body over several days before final closure. This method reduces stress on the baby’s abdominal cavity and lungs.
Post-surgery, babies typically spend several weeks in the neonatal intensive care unit (NICU) to recover and begin feeding.
Life After Surgery: Recovery and Long-Term Outlook
Parents often worry about whether their child will have lasting issues. From real-world cases, here are some observations:
- Feeding and Digestion: Many babies face challenges in the first weeks as their intestines adjust, but most eventually feed normally.
- Growth and Development: With proper nutrition, growth is generally comparable to other children.
- Long-Term Risks: A minority may face bowel obstruction or slower digestion, but these risks decline with age.
Emotional recovery for families is just as important. Support from counselors, nurses, and parent groups helps ease the stress of prolonged hospital stays.
Common Myths and Misconceptions
Misinformation often adds unnecessary fear. Let’s clarify a few myths:
- Myth: Gastroshiza is always fatal.
Reality: Modern medicine has transformed survival outcomes, with most children leading normal lives. - Myth: It’s caused by poor prenatal care.
Reality: While healthy pregnancy practices help, most cases arise without controllable causes. - Myth: Surgery always leaves major disabilities.
Reality: Scarring is minimal, and long-term disabilities are rare when treatment is timely.
Real-Life Stories and Case Insights
One mother shared her journey online: her son was diagnosed with gastroshiza at 20 weeks. With preparation, the baby was delivered at a specialized hospital, underwent surgery, and is now a thriving toddler. Stories like this show that hope, planning, and medical expertise can reshape what first feels like a devastating diagnosis.
Actionable Guidance for Expectant Parents
For families navigating gastroshiza, practical steps can make the journey smoother:
- Choose a Specialized Hospital: Ensure the delivery facility has NICU and pediatric surgery support.
- Prepare Emotionally and Financially: Connect with social workers and support groups for guidance.
- Breastfeeding Support: If direct feeding is delayed, expressed milk can help nutrition in NICU.
- Stay Informed: Reliable medical sources and peer communities reduce anxiety and increase confidence.
Visual Recommendations
- Diagram of gastroshiza vs. normal abdominal wall to help parents visualize the condition.
- Step-by-step infographic of treatment options showing primary vs. staged repair.
- Recovery timeline chart from surgery to first feeding to discharge.
These visuals can simplify complex information for families under stress.
Frequently Asked Questions (FAQs)
Q1: Is gastroshiza the same as omphalocele?
No. In gastroshiza, the intestines are exposed directly, while in omphalocele they are covered by a protective sac.
Q2: Can gastroshiza be prevented?
Currently, there is no guaranteed prevention. Healthy pregnancy habits may lower risk but do not eliminate it.
Q3: Will my child have lifelong problems after surgery?
Most children live normal, healthy lives. Some may experience digestive adjustments early on, but long-term issues are uncommon.
Q4: How long does hospital recovery take?
Typically 4–6 weeks, though it depends on how quickly the intestines begin working after surgery.
Q5: Can a baby with gastroshiza be delivered naturally?
Delivery plans vary. Some doctors recommend cesarean for safer handling, while others support vaginal delivery. It depends on the case.
Conclusion and Call to Action
Facing gastroshiza can feel overwhelming, but knowledge is power. With modern surgery, expert neonatal care, and parental support, outcomes are overwhelmingly positive. Families today are not alone—doctors, nurses, and support communities walk this path alongside them.
If you or someone you know is navigating this condition, start by connecting with medical specialists and trusted support groups. Share your journey, ask questions, and remember: with the right care, a diagnosis of gastroshiza is not the end of hope, but the beginning of a story of resilience.